SIU Director’s Report - Case # 17-OCI-022
Warning:
This page contains graphic content that can shock, offend and upset.
Contents:
Mandate of the SIU
The Special Investigations Unit is a civilian law enforcement agency that investigates incidents involving police officers where there has been death, serious injury or allegations of sexual assault. The Unit's jurisdiction covers more than 50 municipal, regional and provincial police services across Ontario.
Under the Police Services Act, the Director of the SIU must determine based on the evidence gathered in an investigation whether an officer has committed a criminal offence in connection with the incident under investigation. If, after an investigation, there are reasonable grounds to believe that an offence was committed, the Director has the authority to lay a criminal charge against the officer. Alternatively, in all cases where no reasonable grounds exist, the Director does not lay criminal charges but files a report with the Attorney General communicating the results of an investigation.
Information restrictions
Freedom of Information and Protection of Personal Privacy Act ("FIPPA")
Pursuant to section 14 of FIPPA (i.e., law enforcement), certain information may not be included in this report. This information may include, but is not limited to, the following:
- Confidential investigative techniques and procedures used by law enforcement agencies; and
- Information whose release could reasonably be expected to interfere with a law enforcement matter or an investigation undertaken with a view to a law enforcement proceeding.
Pursuant to section 21 of FIPPA (i.e., personal privacy), protected personal information is not included in this document. This information may include, but is not limited to, the following:
- subject officer name(s)
- witness officer name(s)
- civilian witness name(s)
- location information
- witness statements and evidence gathered in the course of the investigation provided to the SIU in confidence and
- other identifiers which are likely to reveal personal information about individuals involved in the investigation
Personal Health Information Protection Act, 2004 ("PHIPA")
Pursuant to PHIPA, any information related to the personal health of identifiable individuals is not included.
Other proceedings, processes, and investigations
Information may have also been excluded from this report because its release could undermine the integrity of other proceedings involving the same incident, such as criminal proceedings, coroner's inquests, other public proceedings and/or other law enforcement investigations.
Mandate engaged
The Unit's investigative jurisdiction is limited to those incidents where there is a serious injury (including sexual assault allegations) or death in cases involving the police.
"Serious injuries" shall include those that are likely to interfere with the health or comfort of the victim and are more than merely transient or trifling in nature and will include serious injury resulting from sexual assault. "Serious Injury" shall initially be presumed when the victim is admitted to hospital, suffers a fracture to a limb, rib or vertebrae or to the skull, suffers burns to a major portion of the body or loses any portion of the body or suffers loss of vision or hearing, or alleges sexual assault. Where a prolonged delay is likely before the seriousness of the injury can be assessed, the Unit should be notified so that it can monitor the situation and decide on the extent of its involvement.
This report relates to the SIU's investigation into the serious injury of a 19-year-old man on January 20, 2017 during his apprehension under the Mental Health Act (MHA).
The investigation
Notification of the SIU
On January 24, 2017 at 10:15 p.m., the St. Thomas Police Service (STPS) reported that the Complainant suffered a serious injury during an interaction with STPS members on Friday, January 20, 2017.
STPS reported that on Thursday, January 19, 2017, the Complainant became involved in a dispute with the CW and threatened suicide. He subsequently left their residence at which time the CW contacted police. Police searched the area, however failed to locate the Complainant. On Friday, January 20, 2017 at about 2:00 a.m., the Complainant returned to his residence and the CW re-contacted police. Police attended the residence and decided to apprehend the complainant under the MHA. The Complainant became combative and aggressive with the officers. The Complainant apparently took punches to the right side of the head while being subdued. The apprehension was witnessed by the CW.
The Complainant was transported to the hospital and was formed[1]. He was released Friday at noon and attended the hospital with a possible concussion. He was later diagnosed with a fractured bone in the right ear.
The team
Number of SIU Investigators assigned: 3
Number of SIU Forensic Investigators assigned: 1
SIU Forensic Investigators responded to the scene and identified and preserved evidence. They documented the relevant scenes associated with the incident by way of notes, photographs, sketches and measurements.
Complainant
19-year-old male interviewed, medical records obtained and reviewed
Civilian witnesses
CW Interviewed
Witness officers
WO #1 Interviewed
WO #2 Interviewed
WO #3 Interviewed
Subject officers
SO Interviewed, and notes and prepared statement received and reviewed[2]
Incident narrative
During the evening of January 19, 2017, the CW called 911 to advise that the Complainant had left the family residence harbouring suicidal ideations. It was disclosed that the Complainant had expressed suicidal thoughts in the past, and he was suffering from mental illness. STPS officers, including the SO, spent several hours searching for the Complainant with no success.
At about 2:00 a.m. the next morning, the Complainant returned to his residence and the CW contacted the SO to advise him of that fact. The SO and WO #1, and later WO #2, attended the residence and attempted to convince the Complainant to go to the hospital to voluntarily be assessed. The Complainant refused and the officers decided to apprehend the Complainant under the MHA as he continued to present as a danger to himself. The Complainant was agitated, and loudly and actively resisted the officers' attempts to take him into custody in order to bring him to the hospital. During the struggle, the Complainant and WO #1 fell onto the Complainant's bed (with the Complainant on top of WO #1), and the Complainant began to reach towards WO #1's duty belt which held the officer's use of force options. With that, the SO delivered two distractionary strikes to the right side of the Complainant's head. The Complainant was then handcuffed and transported to the hospital.
The Complainant was held on the psychiatric ward until later that day, when he was released and diagnosed with a possible concussion. The Complainant returned to the hospital several days later and was diagnosed with a fractured bone in his right ear.
Evidence
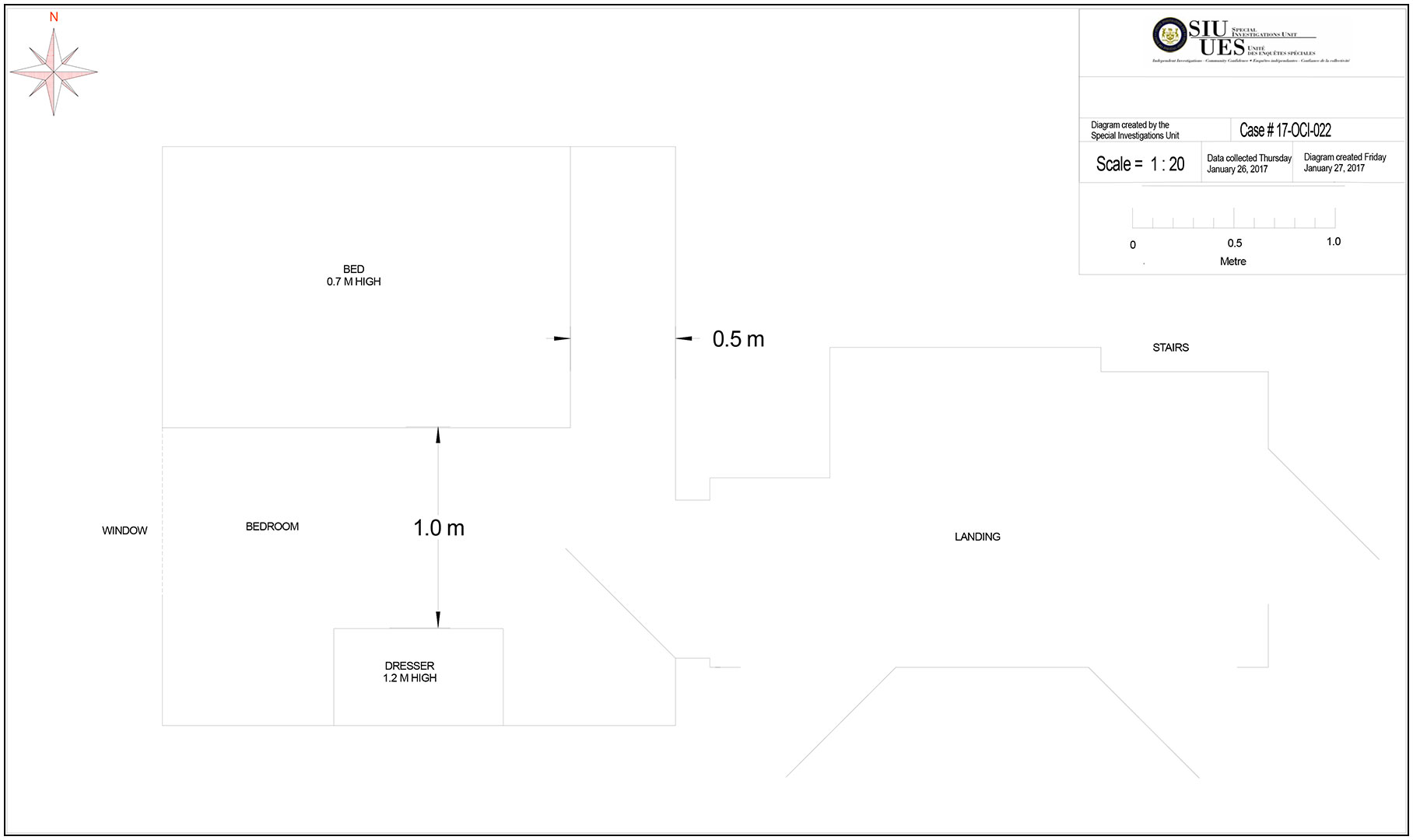
The scene
The Complainant's apprehension was effected in the small (approximately 2.44 metres by 2.89 metres) second floor bedroom he occupied in his family's home in St. Thomas.
Scene diagram
Video/audio/photographic evidence
The SIU canvassed the area for any video or audio recordings, and photographic evidence. The CW provided photos of the Complainant's injuries.
Materials obtained from Police Service
Upon request the SIU obtained and reviewed the following materials and documents from the STPS:
- Communications recordings
- Event Details
- Notes of WO #1, WO #2 and WO #3
- Occurrence report
- Procedure - Arrest
- Procedure - Mentally Disturbed
- Synopsis of Incident
- Training Records – the SO, WO #1, WO #2 and WO #3, and
- Prepared Statements – the SO, WO #1, WO #2 and WO #3
Relevant legislation
Section 17, Mental Health Act - Action by police officer
17 Where a police officer has reasonable and probable grounds to believe that a person is acting or has acted in a disorderly manner and has reasonable cause to believe that the person,
- has threatened or attempted or is threatening or attempting to cause bodily harm to himself or herself
- has behaved or is behaving violently towards another person or has caused or is causing another person to fear bodily harm from him or her; or
- has shown or is showing a lack of competence to care for himself or herself
and in addition the police officer is of the opinion that the person is apparently suffering from mental disorder of a nature or quality that likely will result in,
- serious bodily harm to the person
- serious bodily harm to another person; or
- serious physical impairment of the person
and that it would be dangerous to proceed under section 16, the police officer may take the person in custody to an appropriate place for examination by a physician.
Section 265(1), Criminal Code - Assault
265 (1) A person commits an assault when
- without the consent of another person, he applies force intentionally to that other person, directly or indirectly
- he attempts or threatens, by an act or a gesture, to apply force to another person, if he has, or causes that other person to believe on reasonable grounds that he has, present ability to effect his purpose; or
- while openly wearing or carrying a weapon or an imitation thereof, he accosts or impedes another person or begs
Section 267, Criminal Code - Assault with a weapon or causing bodily harm
267 Every one who, in committing an assault,
- carries, uses or threatens to use a weapon or an imitation thereof, or
- causes bodily harm to the complainant
is guilty of an indictable offence and liable to imprisonment for a term not exceeding ten years or an offence punishable on summary conviction and liable to imprisonment for a term not exceeding eighteen months.
Section 25(1), Criminal Code - Protection of persons acting under authority
25 (1) Every one who is required or authorized by law to do anything in the administration or enforcement of the law
- as a private person
- as a peace officer or public officer
- in aid of a peace officer or public officer, or
- by virtue of his office
is, if he acts on reasonable grounds, justified in doing what he is required or authorized to do and in using as much force as is necessary for that purpose.
Analysis and director’s decision
On January 19th, 2017, the SO was advised by the CW that her son, the Complainant, was missing and suicidal. The SO initiated a search for the Complainant, which was conducted over several hours, with police officers attending at various train trestles as a result of the Complainant having sent out messages on social media implying that he intended to take his own life and having indicated in the past that he intended to do so by way of jumping off of a train trestle. The Complainant first attended one train trestle, where he observed a police officer apparently looking for him, and he hid; he then attended a second train trestle where he observed another police officer and he again hid. As his attempts to gain access to a train trestle to possibly carry out his suicidal intentions were foiled by the presence of police, the Complainant decided to return home.
Once the Complainant arrived back at his home, the CW contacted the SO to advise him of her son's return as she was aware of the ongoing search. The SO and WO #1 attended at the home in an effort to assess the Complainant's mental state and to obtain mental health assistance for him, if necessary. On all of the evidence, from both the civilian and police witnesses, it is not in dispute that the Complainant was neither agreeable to speaking with the police, nor to speaking with a mental health worker or attending at the hospital, with all options being presented to him by the SO and WO #1. The Complainant was both resistant to the efforts of police to get him some mental health assistance and to being assessed. The Complainant does not dispute that he was verbally non-compliant, used foul language, and was verbally aggressive and abrasive. Once police determined that the Complainant was not going to be cooperative, a call was made for assistance, and a third police officer, WO #2, attended. The Complainant was apprehended pursuant to the MHA and transported to hospital, where he was committed on a Form 1 under the MHA by the attending physician on the basis that he was a danger to himself. Following his discharge, the Complainant re-attended at the emergency room and it was discovered that he had suffered a fracture of the Mastoid Process (located in the posterior portion of the temporal bone behind the ear, the mastoid process provides an attachment for certain muscles of the neck) of his right ear.
The Complainant, in his statement to investigators, confirmed the above facts as accurate. The Complainant alleges that after he was put down onto the bed by the officers, face down, he felt the handcuffs being placed on his hands, while he was still face down, and then felt punches land on the right side of his head, by the back of his ear, and on his jaw. The Complainant was unsure as to which officer struck him. The Complainant denied hitting, kicking or physically fighting any of the officers. In her interview, the CW identified WO #2 as the officer who punched the Complainant with at least two downward swings with his right fist, hitting the back of the Complainant's head, neck and shoulder area.
During the course of this investigation, two civilian witnesses, including the Complainant, and all three of the police officers present at the Complainant's home, including the SO, were interviewed. All police witnesses also provided their memorandum book notes and their prepared statements for review. Additionally, investigators had access to the police radio transmissions recordings and the medical records of the Complainant.
The Complainant's medical records confirm that on January 20th, 2017, he was seen at the hospital and was involuntarily committed on a Form 1 under the MHA, after consultation with the on-call psychiatrist, on the basis that the doctors were of the view that the Complainant was a danger to himself and that he had underlying mental health issues. The notes indicate that "[the Complainant] self-admittedly is not safe. He tells me that he has suffered depression and will not contract for safety.[3] He was quite polite and demonstrated some insight here in the Emergency Department. He said he struggled with thoughts of depression and suicide for some time. I was able to contact [name of the psychiatrist on call]. We are in agreement that the Complainant should be admitted to the Psychiatric Unit for observation and be placed on a form." Later on in the records the doctor further noted, under Provision Diagnosis: "Suicidality and Depression", and under Plan: "[the Complainant] will require admission for observation to the Mental Health Ward. He is a threat for self-harm". While the records from the following date indicate that the then on-duty psychiatrist, who was the Complainant's regular psychiatrist and who had dealt with him many times in the past, discharged the Complainant, he indicated in the records that he had requested the Complainant to voluntarily remain in the Psychiatric Unit for a longer time, but that the Complainant refused, as a result of which he was discharged.
When the Complainant returned to hospital on January 24th, 2017, his version as to how he was injured was recorded on his medical records as follows:
According to Pt [patient] was assaulted by police four evenings ago. Was threatening to kill self so police were called by mom – used force to bring to ED [Emergency Department] as pt was resistant. Pt states was kneed in R side of head multiple times.
The SO advised that when he and WO #1 attended at the residence, they did so in order to assess the Complainant's mental condition. He advised that he explained to the Complainant that this was why the police were present and tried unsuccessfully to get the Complainant to discuss his thoughts of suicide, but the Complainant became agitated and repeatedly referred to the officers as "pigs" and used various profanities towards them. This evidence is consistent with the observations of WO #1 who described the Complainant using profanities towards both police officers while the SO tried to facilitate a conversation with the Complainant. WO #1 advised that he too explained to the Complainant why police were there and that their interest was only as to the well-being of the Complainant, in that they wanted to provide him with some treatment options. Despite repeated efforts, the SO was unable to calm the Complainant, who repeatedly told the police officers to leave. WO #1 described the conversation with the Complainant as running in a loop, with the police officers providing explanations and options to the Complainant and the Complainant responding with profanities and disinterest. WO #1 advised that the Complainant's anger did not make sense to him and he wondered if the Complainant was under the influence of marijuana, which he could smell in the room; the Complainant would not communicate with either of the police officers or the CW. WO #1 recalled the Complainant stating that "if you fucking touch me, we're fucking fighting." WO #1 considered and rejected his Conducted Energy Weapon (CEW) as an available use of force option to apprehend the Complainant.
When the Complainant sat up on the edge of the bed, the SO advised that he took a step back for safety and the Complainant became increasingly agitated, asking the CW why she had let these "pigs" in the house. The SO spoke to the Complainant for four to five minutes, but made no progress, and he decided that he would apprehend the Complainant under the MHA. WO #1 called for assistance. WO #1 advised that his hopes were that the presence of three police officers might de-escalate the situation, or, in the alternative, the SO advised that a third officer would either calm the Complainant, or assist with his apprehension, if he resisted.
Upon WO #2's arrival, WO #1 advised that it was decided among the officers that they would use necessary force to apprehend the Complainant and have him assessed under the MHA. The SO and WO #1 both advised that they then requested the CW step out of the bedroom for her own safety. The SO advised the Complainant that he was being apprehended under the MHA and would be transported to hospital; he then told the Complainant to stand up, and he complied. The SO moved in front of the Complainant and took control of his right arm by grasping the Complainant above the elbow with his left hand, and grasping his wrist with his right hand. The SO advised that the Complainant immediately resisted and pushed the SO back toward the window on the west wall. The SO then spun the Complainant, while holding onto his right arm, and pushed him into the corner between the dresser and the window while WO #1 assisted by holding the Complainant's left arm.
WO #1 described himself and the SO wrestling with the Complainant in an attempt to get him down on the bed in order to handcuff him and, during the struggle, they came dangerously close to a tall, low, shin height window and WO #1 was concerned that they might fall through the window. WO #1 described the three of them as pushing and pulling each other and WO #1 tried to put the Complainant in a headlock using his right arm and attempted to twist the Complainant onto the bed. During the struggle, however, WO #1 was flipped onto his back and onto the bed and the Complainant broke away from him and was now on top of WO #1.
The SO advised that he gave commands for the Complainant to stop resisting, and he observed the Complainant push out from the corner, causing WO #1 to fall backwards onto the bed with the Complainant on top of him. The SO described WO #1 and the Complainant as being chest to chest. The Complainant was squirming and WO #1 had control of the Complainant with his right arm wrapped around his head in the centre of the bed. The SO then lost control of the Complainant's right arm and observed that the Complainant had his right arm between his body and that of WO #1, in the area of WO #1's duty belt with his use of force equipment. The SO attempted to pull the Complainant's arm out and put it behind his back for handcuffing and he directed the Complainant again to stop resisting and to surrender his arm. The SO advised that at that point he was concerned that the Complainant could grab one of the use of force options from WO #1's duty belt.
WO #1 advised that his mind also went to the exposure of his use of force equipment to the Complainant in that position, and he described the Complainant as being on his knees, with his hands on WO #1's bullet-proof vest, and then pushing his hands against WO #1's vest, as if pushing himself up and off of the bed. WO #1 yelled at him to stop resisting. At that point, the SO considered employing one of his own use of force options, but rejected all of them due to the close quarters and the fact that he could inadvertently injure one of the other officers. The SO opted to punch the Complainant instead, with a closed right fist to the right side of the Complainant's face, using about 60-70 percent of his strength; he further described the blow as being delivered from a distance of 18 to 24 inches [45 to 61 centimetres]. WO #1 advised that he saw the SO use a closed fisted hand to hit the Complainant on the right side of his head. Both the SO and WO #1 described the blow as unsuccessful and the Complainant did not surrender his arm.
WO #1 advised that he tried to pull the Complainant, by whatever means possible, back down onto the bed and, through the efforts of the SO and himself, the Complainant was pushed face down onto the bed and WO #1 managed to get off his back and onto his knees beside the Complainant. WO #1 positioned himself so that his right knee was pushed on the Complainant's back and shoulder area to hold him down, while the Complainant continued to squirm and try to push himself off the bed. The SO continued to issue commands to the Complainant to stop resisting and surrender his arm. After about five seconds, the SO delivered a second punch with the same amount of force as the first and to the same area. The SO described both punches as striking with the first two knuckles of his right fist landing on the Complainant's face. WO #1, who observed both punches, described them as a closed-fisted punch to the right side of the Complainant's neck, near his ear, and opined that it was similar to how they were trained to deliver a brachial plexus-tie-in strike. This second punch was effective and the SO was able to secure the Complainant's right arm and the Complainant was handcuffed. WO #1 advised that when the SO delivered the two closed-fisted blows to the Complainant, WO #1 had a view of the doorway and he did not see the CW, although he knew that she was in the area. WO #1 estimated that the Complainant was handcuffed approximately ten to fifteen seconds after the SO had delivered the second blow. WO #1 himself did not hit the Complainant at any time during the struggle to handcuff him. The SO also advised that at no time did any other officer strike the Complainant and, once the Complainant was handcuffed, he immediately stopped resisting and no further force was used by anyone. The SO estimated that the entire struggle lasted about 30 seconds, during which his handcuff key, his flashlight, and the keys to his police vehicle were all dislodged from his uniform and fell somewhere on the floor. As the SO escorted the Complainant from the bedroom, he observed the CW in the doorway of another bedroom about eight feet [2.44 metres] from the Complainant's bedroom door.
WO #1 advised that as they were escorting the Complainant out the front door to the police cruiser, he asked the Complainant which shoes were his and the Complainant responded "fuck you, you fucking pigs" and, as such, he was removed from the house without his shoes.
Upon arrival at the hospital, the Complainant asked the SO if he, the Complainant, had a bruise on the right side of his head, and the SO saw some redness behind the Complainant's ear and neck in the general area where he estimated he had struck the Complainant.
WO #2 advised that he was still in the hallway when the CW exited the bedroom and tapped him on the shoulder and then whispered to him that she thought that the Complainant smelled of marijuana. WO #2 then heard a struggle in the bedroom and he entered the room and observed the SO attempting to gain control of the Complainant. He indicated that the Complainant had stood up and was actively resisting the attempts to control him. He also observed the SO and WO #1 move with the Complainant toward the right side of the bed, where WO #1 bounced off a curtained window with enough force that WO #2 thought he might be pushed through the window. WO #1 then tried to get the Complainant into a headlock while the SO tried to gain control of the Complainant's right arm, and the three moved toward the corner of the room where WO #2 joined in the struggle, by grasping the Complainant's left forearm, and the Complainant was turned and pushed onto the bed but WO #1 landed on the bed underneath the Complainant. WO #2 advised that the Complainant yelled that he could not breathe and that he was the officer who told the Complainant that he could breathe just fine if he was able to speak. WO #2 then successfully secured the Complainant's left hand behind his back, while the SO secured his right, and he was handcuffed and then assisted to his feet and escorted from the room by the SO and WO #1. WO #2 advised that he at no time struck the Complainant.
Following the Complainant being escorted from the room, WO #2 and the CW searched the floor and located a handcuff key, a police vehicle key fob, and a flashlight under the bed.
WO #2 indicated that once at the hospital, he was the police officer to whom the CW indicated that the Complainant was upset with the amount of force used during his apprehension and he, WO #2, was the officer who told her words to the effect that the police had done what they needed to do to take the Complainant into custody. WO #2 also indicated that the CW showed him a picture on her cell phone of what appeared to be a suicide note from her son.
WO #2 advised that at no time did he consider that the police should have just walked away from the Complainant, as he believed that the situation was still volatile, that the Complainant was "amped up", and he was upset with both the CW and the police. He described the Complainant as still being in some sort of emotional crisis.
On a review of all of the evidence, I have some difficulty in reconciling the statement of the Complainant to SIU investigators, which was provided on January 25th, 2017 wherein he described being punched twice in the head and then admitted that the CW told him it was WO #2 who had punched him in the head, with his statement to medical staff, as recorded in his medical notes on January 24th, 2017, wherein he stated he had been "kneed in R side of head multiple times." On this basis, it appears that the Complainant did not know how he received his injury, but may have simply taken the CW's version as his own.
In addition, I have some difficulty with the CW's initial statement in that she indicated first that when she exited the bedroom she exchanged places with WO#2, who then entered the bedroom, which statement I accept as accurate as it confirms the evidence of all three police officers, but she later indicated that it was not until after the Complainant had been handcuffed that WO#2 then ran from the hallway into the room and took at least two downward swings with his right fist hitting the back of the Complainant's head, neck and shoulder area. The first version, that being that she exchanged places with WO#2, who then entered the bedroom as she exited into the hallway, before any efforts to apprehend the Complainant were carried out, confirms the evidence of WO#2, who advised that other than the CW being out in the hallway with him for a matter of seconds while she whispered in his ear that she believed her son may have smoked some marijuana, he was in the bedroom for the entirety of the struggle and that the Complainant was not handcuffed when he entered. Additionally, I find it difficult to believe that the CW, from out in the hallway, could have determined when exactly the Complainant was actually handcuffed, when she described the struggle as a pile of people with little movement other than shuffling toward the window. Furthermore, WO #1 advised that he had a view of the doorway when the SO struck the Complainant, and he indicated that the CW was not visible when the two blows were struck and, when he escorted the Complainant out of the room, the CW was in the doorway of another bedroom some eight feet [2.44 metres] down the hall.
I also find that the statement of the CW appears to be missing some of the sequence of events inside the bedroom which was provided by the Complainant himself, regarding his struggling with the officers and grabbing onto their shirts, which appears to confirm the evidence of WO #1 as to the Complainant grabbing onto WO #1's vest, while the statement of the CW is completely silent in this regard.
I also interpret the fact of the handcuff key, the flashlight, and the car keys being found in and under the bed, after they were dislodged from the SO's uniform, as corroborating the evidence of the three police officers as to the degree of the struggle between the Complainant and the police officers.
Finally, the CW's firm assertion that WO #2 struck the Complainant twice in the head is directly contradicted by all three police officers; with WO #2 adamantly denying that he ever struck the Complainant and the SO openly admitting that he was the officer who struck the blows. WO #1 corroborated the evidence of both officers in that he observed the SO delivering the two closed-fisted strikes to the Complainant's head. I can see no logical reason why all three of these officers would lie as to who struck the blows, while openly admitting that two blows were indeed struck by one of the police officers during the apprehension resulting in the serious injury to the Complainant. Furthermore, I note that the SO noted in his notebook, which he appears to have completed before the end of his shift on January 20th, 2017, that he "punched [the Complainant] in head to gain compliance". These notes were completed prior to the Complainant having been assessed with a serious injury on January 24th, 2017, following which the SIU was notified and the investigation launched. As such, I accept that these notes provide further confirmation that the two blows to the Complainant's head were delivered by the SO and not by WO #2, as alleged by the CW.
On the basis of these significant inconsistencies in the evidence of both the Complainant and the CW, that being the Complainant's lack of knowledge as to how his injury was caused, and by whom, and the CW's clearly inaccurate allegation as to when the punches were delivered and by whom, I find that I have serious difficulties with the version of events as provided by both the Complainant and the CW and, as such, I do not accept that the Complainant was punched twice in the head by WO #2 nor do I accept that the injury was inflicted after he was handcuffed.
On the credible evidence remaining, then, I find that I have reasonable grounds to believe that during the struggle to handcuff the Complainant, in order to apprehend him under the MHA and transport him to hospital to be assessed, he was struck in the head twice by the SO, which resulted in the Complainant's serious injuries. On these facts, the question that remains is whether or not there are reasonable grounds to believe that the SO, in delivering these two blows, committed the offence of assault causing bodily harm contrary to s. 267(b) of the Criminal Code.
Pursuant to section 25(1) of the Criminal Code, police officers are restricted in their use of force to that which is reasonably necessary in the execution of a lawful duty. Turning first to the lawfulness of the Complainant's apprehension, it is clear based on all of the information provided to the SO by the CW with respect to the Complainant's messages on social media, prior threats of suicide, prior behaviour and his mental health issues, it was not unreasonable for the SO to believe that there were grounds, pursuant to s.17 of the MHA, to apprehend the Complainant as a danger to himself. The MHA provides that:
s.17 Where a police officer has reasonable and probable grounds to believe that a person is acting or has acted in a disorderly manner and has reasonable cause to believe that person,
- has threatened or attempted … to cause bodily harm to himself …
and in addition the police officer is of the opinion that the person is apparently suffering from mental disorder of a nature or quality that likely will result in,
- serious bodily harm to the person …
and that it would be dangerous to proceed under section 16, the police officer may take the person in custody to an appropriate place for examination by a physician.
I note that the language of s.17 relies heavily on the judgment of the police officer, in that it refers to the officer's "reasonable and probable grounds," his "opinion," and his finding that it would be dangerous to wait, pursuant to s.16, to get a court order to apprehend the person. In the circumstances of this case, I can find no fault in the SO's belief that he had "reasonable and probable grounds" to believe that the Complainant had threatened to cause bodily harm to himself based on the information provided to him by the CW, as well as her own belief that her son was going to take his own life. Furthermore, based on that same information, there was ample evidence upon which the SO could form the opinion that the Complainant suffered from a mental disorder of a nature or quality that likely would result in serious bodily harm to himself. I also find that the expert opinions of the emergency room doctor who assessed the Complainant, and the on-call psychiatrist who was consulted, that the Complainant posed "a threat for self-harm" and therefore met the requirements to be involuntarily committed to hospital on a Form 1 under the MHA, further confirmed the actions of the SO when he apprehended the Complainant on that very basis.
I can fully appreciate how an apprehension under the MHA is one duty for which police cannot hope to garner everyone's approval. If a party is apprehended and then released from hospital, the actions of police in apprehending him is subject to criticism. If a party is left and not apprehended and subsequently takes his own life, the actions of police in walking away would be the subject of even more strenuous criticism. As such, I cannot find fault with the SO's erring on the side of caution, especially where the information provided by the CW was so compelling, and where the alternative of walking away and leaving the Complainant without the help which he so obviously needed could have had tragic consequences. On the evidence available to the SO on the night in question, I can find no fault in his reasoning that he had the necessary grounds pursuant to the MHA and, as such, the apprehension of the Complainant was legally justified in the circumstances.
I turn, then, to the amount of force used by the SO when he twice delivered a closed-fisted punch to the side of the Complainant's head. While the Complainant described the punches as being a nine and one half out of ten on a scale of how much force was used, I am not inclined to accept that assessment for a number of reasons, including: that the Complainant was apparently unable to differentiate whether or not he was even punched or kneed (particularly since the amount of force which could be generated in the confined quarters by a knee strike would be far less than what one could deliver in a closed-fisted punch); that the Complainant apparently showed no reaction to the first punch and continued to struggle and resist; and, that WO #1 and the SO both assessed the punch as being closer to 60 or 70 percent of a full strength blow; and finally, if he was hit as hard as the Complainant alleges, I do not accept the fact that the Complainant would have reacted in the manner he claims. That is he claims he laughed and asked if they were going to hit him again. Moreover, I doubt that it is possible for the person receiving the blow to accurately estimate how forceful the blow was, when he is unfamiliar with the strength of the person delivering the blow. In this regard, I accept that both WO #1, but more specifically the SO, would have been in a far better position to assess the force behind the blow, than would the Complainant.
I have also considered the observation of WO #1 that the blows delivered by the SO were similar to a technique that police are trained to deliver, that being a brachial plexus-tie-in strike. After some on-line research, as well as making enquiries as to techniques taught to training police officers, I have been able to confirm that the brachial plexus-tie-in strike is indeed taught at many police colleges and by the military, as well as being a technique taught in self-defence classes and in martial arts, but most significantly by both the Ontario Police College and the Toronto Police College. As I understand it, this technique involves striking in the area of the side of the neck below the ear which is meant to shock the carotid artery, jugular vein and vagus nerve in order to distract and/or immobilize the subject. It is unclear to me, however, on the evidence, whether or not this was actually the technique that the SO meant to deliver since the SO indicated that he believed that both blows landed on the Complainant's face and not below his ear, which is where they actually landed.
On the evidence from both WO #1 and the SO, both officers considered their use of force options and rejected them for various reasons. Having done so, the SO was of the view that one of the only options remaining open to him was to use a closed-fisted blow to the head/face area. This was not unreasonable taking into account that once the decision was made to apprehend the Complainant, the ensuing struggle between the Complainant and the officers became a fluid and fast-moving situation in a very confined space wherein the options available to the police officers were very limited. Both WO #1 and WO #2 indicated that they became concerned, during the struggle, that WO #1 might go out through the window due to the amount of force with which he was pushed against the window. When WO #1 landed on his back on the bed with the Complainant on top of him, both WO #1 and the SO also became concerned that the Complainant had access to WO #1's use of force options. Finally, when the Complainant continued to struggle and resist, and pushed himself up off of the bed, I find the SO's assessment that there were very few remaining options available to him, and that he had to act quickly, was reasonable in the circumstances. Furthermore, the fact that the first blow delivered by the SO yielded no reaction, and did nothing to lower the Complainant's resistance, would lead one to believe that the blow was not as forceful as opined by the Complainant and apparently led the SO to believe that he needed to deliver a second blow in order to finally bring the struggle to an end.
Although I find that the Complainant's injury was caused by the SO delivering two closed-fisted punches to the Complainant's head, I find that pursuant to section 25(1) of the Criminal Code, the officer used no more force than was reasonably necessary in the execution of his lawful duties in apprehending the Complainant in order to get him the medical attention that the officers' reasonably believed he needed. On all of the evidence, I am unable to determine whether the SO intended his blow to land on the Complainant's face or if he was attempting to strike the Complainant below the ear as per the technique described earlier, what is clear, however, is that with the struggling and resistance of the Complainant, one or both of the blows did not land as intended and the Complainant subsequently sustained his injury.
In finding that the SO's actions did not contravene s.25(1), I have fully considered the state of the law as set out by the Supreme Court of Canada in R v Nasogaluak, [2010] 1 S.C.R. 206, as follows:
Police actions should not be judged against a standard of perfection. It must be remembered that the police engage in dangerous and demanding work and often have to react quickly to emergencies. Their actions should be judged in light of these exigent circumstances. As Anderson J.A. explained in R. v. Bottrell C.C.C. (2d) 211 (B.C.C.A.):
In determining whether the amount of force used by the officer was necessary the jury must have regard to the circumstances as they existed at the time the force was used. They should have been directed that the appellant could not be expected to measure the force used with exactitude. [p. 218]
On this factual scenario, while I accept that it was a judgment call whether or not to apprehend the Complainant, once that course had been embarked upon, and the Complainant, by his struggling and resistance, put the safety of WO #1 at risk, it was incumbent upon the other officers to come to his aid and to bring the struggle to an end. With very few, if any, other options available, I find that the SO's resort to physical force to bring the struggle to an end was reasonable in the circumstances and I can find no evidence to support the conclusion that he intended the injury that was subsequently sustained when the blow did not land as predicted. In this regard, I have further considered the decision of the Ontario Court of Appeal in R. v. Baxter (1975), 27 C.C.C. (2d) 96 (Ont. C.A.), that officers are not expected to measure the degree of their responsive force to a nicety.
On all of the evidence, including that of the Complainant and the CW, there is no question that the officers showed both concern and patience in trying to convince the Complainant to voluntarily speak to a mental health crisis worker by any means he wished, while the Complainant had absolutely no intention of having his mental health assessed. Whether or not the Complainant's resistance and agitation with the police officers was due to their having interfered with his plans is a question that cannot be answered in the circumstances. It is clear, however, that the actions of the SO and WO #1 progressed from patience and negotiation, to a decision to apprehend, and finally, to physical force in order to subdue the Complainant. There is no question that had the Complainant gone with the officers without a struggle, he would not have been injured. The actions of the police officers progressed in a measured and proportionate fashion to meet and overcome the resistance of the Complainant, and the SO did not resort to delivering the two blows to the Complainant until WO #1 was put at risk by the actions of the Complainant.
In the final analysis, while the injury to the Complainant was unfortunate, I am satisfied that it was not the result intended by the SO, but rather was an unfortunate result of the resistance and struggling of the Complainant. On these facts, I am satisfied that there are reasonable grounds to believe that the actions exercised by the officers fell within the limits prescribed by the criminal law and there are no grounds for proceeding with charges in this case.
Date: January 10, 2018
Original signed by
Tony Loparco
Director
Special Investigations Unit
Endnotes
- 1) [1] A Form 1 under the MHA allows a physician to hold an individual in a psychiatric facility for up to 72 hours to undergo a psychiatric assessment. [Back to text]
- 2) [2] The SO was originally designated as a Witness Officer. The SIU received a copy of his duty notes and a will-say statement. When the investigation revealed the SO may have caused the Complainant’s injury, he was, before being interviewed, re-designated to Subject Officer and his notes and will-say were returned/destroyed. The SO, after being re-designated to a Subject Officer, volunteered to be interviewed in this matter and provided his notes and will-say statement to assist the investigation. [Back to text]
- 3) [3] Hospitals require that a person who has indicated suicidal ideations be requested to sign a contract with the hospital that they will not self-harm, before they can be released. This is meant to deter the person from taking their own lives as they have promised that they would not do so. [Back to text]
Note:
The signed English original report is authoritative, and any discrepancy between that report and the French and English online versions should be resolved in favour of the original English report.